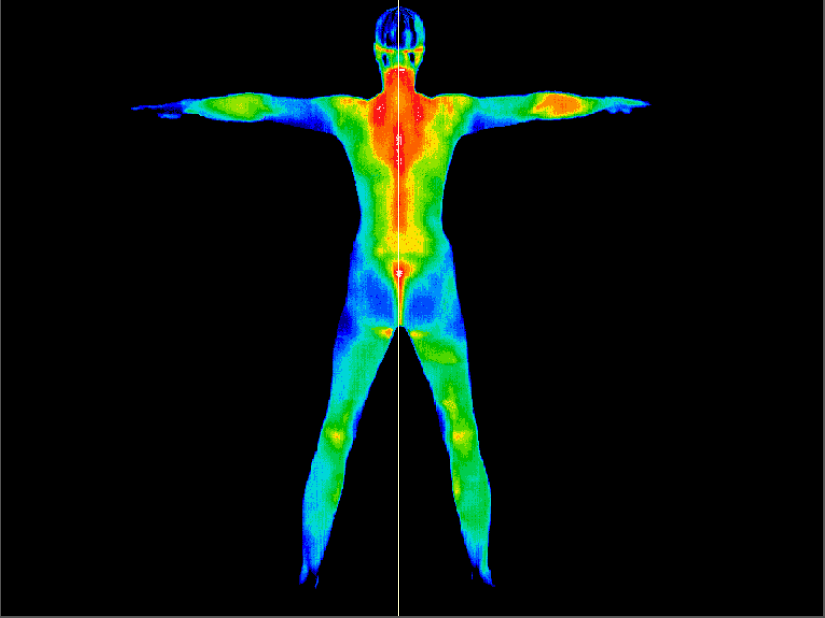
Partial or whole-body thermography is an excellent tool in sports medicine and pain management because it can map inflammation from neurologic or musculoskeletal dysfunction.
Thermography uses infra-red photography to measure thermal emissions from the skin and subcutaneous tissue. The thermograph is the picture produced. It provides a visual means of identifying areas of inflammation.
It can help determine where your pain is coming from and the best way to treat it. Prompt and more effective treatment may be initiated so that full blown, difficult to manage, chronic disability may be averted.
X-rays, ultrasound, and MRIs are all tests that provide information on the structures found within the body. Thermography is the only imaging technology at this time that is capable of showing physiological changes and metabolic processes. Thermography can often show where the pain is coming from. And there is no exposure to x-rays, nothing to prompt claustrophobic feelings.
Thermography is useful for detecting and monitoring many conditions including:
- Vein Conditions (deep vein thrombosis, for example)
- Fibromyalgia
- Visceral Dysfunction
- Carpel Tunnel Syndrome
- Chronic Low Back Pain
- Headache / Sinus Pain
- Neck and Back Problems
- Referred Pain
- Repetitive Strain Injuries
- Whiplash
- Arthritis
- Skin Cancer
- Arthritis
- Chronic Nerve Injury
- Sports Injuries
Posttraumatic pain is often associated with complex disturbances of the sympathetic nervous system which also controls microcirculation of the skin. Circulatory skin changes are in turn reflected by altered superficial thermal emission, which can be reliably imaged by thermography. Thermographic findings often appear before skin or roentgenographic changes become manifest and lead to earlier diagnosis.
The controlling mechanism for thermal emission and dermal microcirculation is the sympathetic nervous system. There is a persistent vasomotor tone in the peripheral arterioles and precapillary sphincters. This tone allows the dermal vessels to stay in a partially constricted state so as to inhibit excess heat loss from a higher core temperature. The autonomic regulation involves synapse of preganglionic sympathetic fibres to postganglionic. The postganglionic fibres travel to vascular structures and modulate alpha receptor function in the dermal microcirculation. When there is increased sympathetic function vasospasm will occur due to further vessel constriction and there will be decreased thermal emission at the cutaneous level. This may occur due to either increased postganglionic fibres function/irritation or hypersensitization of the alpha receptors in the dermal microcirculation allowing increased binding of catecholamines. Increased thermal emission will conversely be seen due to situations of decreased postganglionic function (such as seen in denervation) or alpha receptor blockade (receptor fatigue due to release of vasoactive substances such as substance P).
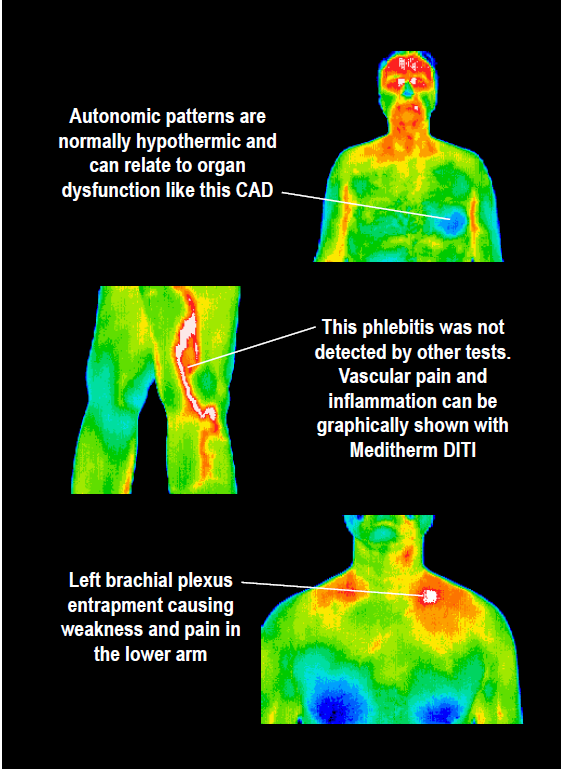
Much research has been done documenting referred pain in myofascial syndromes and somatic visceral conditions. These referred pain zones are believed to be a somatocutaneous sympathetic response. They work via a common autonomic neural network. The somatosympathetic response can be imaged by Thermography. Pain is believed to be a neurogenic and autonomic response to injury and DITI findings have been found to correlate well to the patient’s report of painful areas and is well suited for diagnostic purposes in athletic injuries. Thermography is not a picture of pain, however it is a picture of autonomic dysfunction which seems to correlate well with regions of pain.
Thermography is a diagnostic tool in the differential diagnosis of neuromusculoskeletal injuries – commonly foot and ankle, knee, shoulder, and lumbar and cervical spine – and their prognosis for return to participation and/or competition.Thermography has been recognized as a viable diagnostic tool since 1987 by the AMA council on scientific affairs, the ACA council on Diagnostic Imaging, the Congress of Neurosurgeons in 1988 and in 1990 by the American Academy of Physical Medicine and Rehabilitation.
The length of your appointment depends on the type of scan you desire. One area of interest, such as a knee scan, could require 3-5 images and may take 15 minutes to complete. A full body scan, with many images, may take 60 minutes to complete.